


Impressions from the 2024 American Psychiatric Conference
Also a food blog, music review, and observations on the NYC marijuana scene.

I went to the American Psychiatric Association’s (APA) conference in NYC this weekend, and because I’m still wrestling with my next deep-dive psychopharm piece, I decided to write down my impressions of the conference. This was the first APA main conference I’ve been to (I’ve attended their off-cycle Mental Health Services Conference in NYC twice before). I mostly went to speak with potential employers at the expo hall, not so much for the presentations.
Outside:
As is usual for these sorts of things, there was a large group of protesters holding up signs demanding that we stop “torturing” people with ECT. My understanding is that the majority of these individuals are actually Scientologists, which has had a vendetta against psychiatry ever since L. Ron Hubbard revealed to the world in his science fiction novels that the schizophrenics were right all along about mental illness. Not that mental illness doesn’t exist – L. Ron definitely thought it did – but that it’s actually caused by alien spirits that roam the Earth and live in human bodies after an intergalactic warlord called Xenu shipped billions of human beings who were his enemies and used volcanos and hydrogen bombs to murder them. Also you can cure these problems by paying the church of scientology thousands of dollars to level up your control over these spirits1. I’m not joking.
On a more serious note, it really made me wonder if any of the protestors had met anyone who has had ECT in the last 20 years, because modern ECT methods are just so incongruent with what they think the modal patient experience with ECT is. It’s also, you know, an incredibly effective and lifesaving treatment for certain patients.
The Expo Hall:
I was a little surprised to see the Amen Clinic there. For those of you not in the know, the Amen Clinic is a company run by Dr. Daniel Amen that relies very heavily on the use of a type of PET scan called SPECT (single photon emission computed tomography) to “diagnose” and treat patients who may have mental illness but also may just happen to have some SPECT results that look weird. They also happened to be selling three different supplements for “brain health,” because of course they are. As far as I can tell, the Amen Clinics are mostly a scam and prey on uninformed consumers who think that other psychiatrists aren’t using SPECT BRAIN IMAGING because they’re just not sophisticated enough. The actual reason we’re not using SPECT BRAIN IMAGING is that it doesn’t actually seem to provide any clinical benefits and is pretty much just a waste of money.
I say “surprised” here because the APA Conference is mostly (almost exclusively?) attended by psychiatrists, who are generally smart enough to have a dim view of snake-oil salesmen like the Amen Clinic, and so I wouldn’t think that Amen would get much mileage out of their booth. I’m also a little surprised that the APA would want to affiliate themselves with the Amen Clinic and allowed them to have a booth, though I don’t know what (if any) policy they have for who their exhibitors can be.
I went around to quite a few employer booths. Most of them were advertising for locations that I had no interest in. The places I did speak to were staffed by nice people, but I think as soon as they heard that I was a PGY-3 they mostly lost interest in talking to me about specifics. From my point of view, it’s a bit of a shame; my impression is that most PGY-4s have jobs lined up by now, so waiting till May speak to employers is just too late.
About half of the expo floor was dominated by pharmaceutical companies shilling their latest drugs. In general, I was unimpressed. Good News! the Vraylar booth said, the majority of patients on our medication at 6 months didn’t have a >7% increase in weight! What’s the percentage… uh, well, 81%. So your new, more expensive, just-as-efficacious-as-aripiprazole antidopaminergic has weight gain side-effects that are pretty much identical to… aripiprazole. Yikes.
The people selling viloxazine (Quelbree) announce that they are “Today's #1 prescribed branded non-stimulant ADHD medication,” but I’m pretty sure that they are literally be the only branded non-stimulant ADHD medication on the market at the moment. They were also excited to mention that they are the first novel approach to ADHD treatment on the market in a decade. First, are they just trying to gaslight us into forgetting that atomoxetine exists? Second it’s a selective norepinephrine reuptake inhibitor that was originally marketed in Europe as an antidepressant in 1974, but was a commercial flop and was pulled from markets in 2002. There is nothing new about Quelbree.
I did not to talk to any of the Bupropion/Dextromethorphan people (Auvelity) but did enjoy their strawberry lemonade.
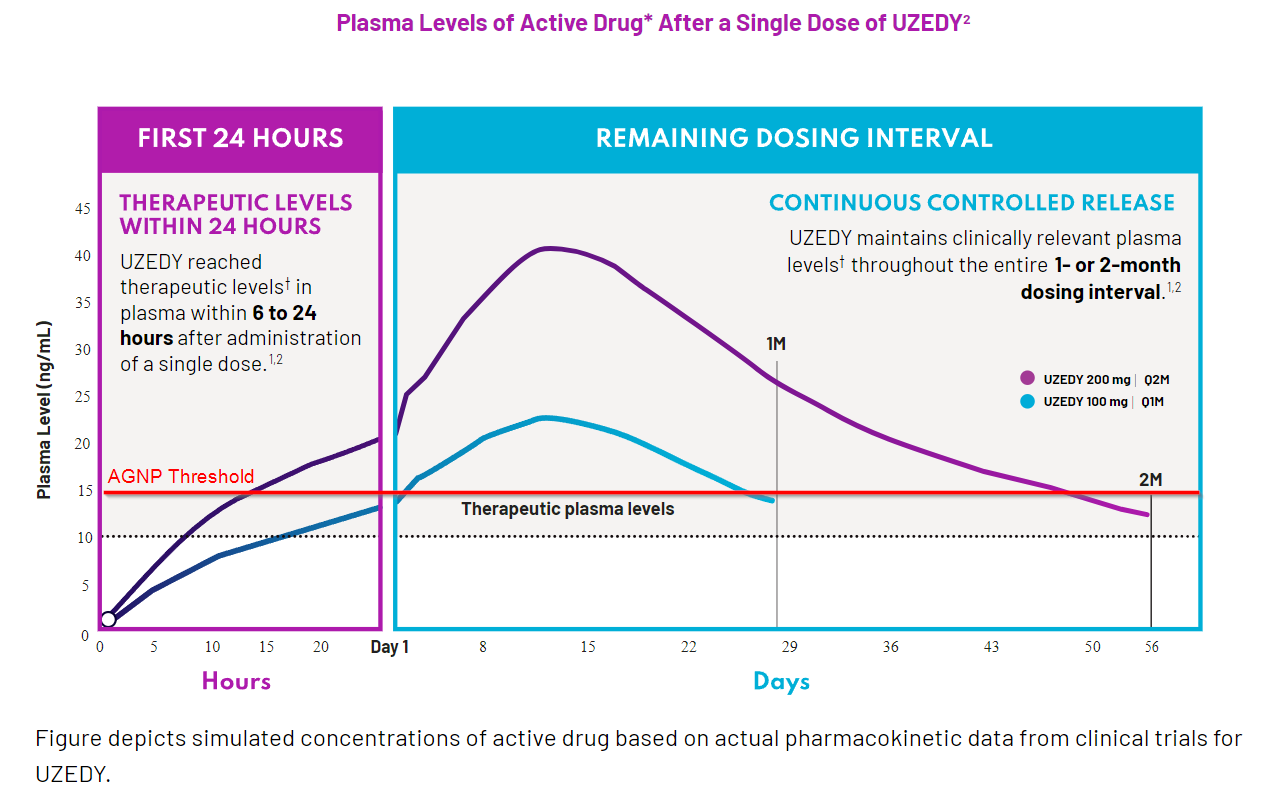
The only actually cool and useful pharmaceutical I saw was called Uzedy2 which is a relatively new long-acting injectable (LAI) version of risperidone. Wait, you say, I am very up to date on my pharmaceuticals and this isn’t new at all! Aren’t there already like three other risperidone LAIs on the market already?
Yeah, but this one you might actually use instead of paliperidone.
It’s subQ, reaches therapeutic levels within 24h of administration, does not require a loading dose or PO supplementation, can be given once or twice a month, and you don’t have to wait for 3 injections before you step up to q2month formulation. Most importantly, it has RISPERIDONE MOLECULE3

Those of you who aren’t psychiatrists probably don’t see what the big deal is, and individually I don’t think any of these things would be all that special. The fact that you get all of this in a single package is what makes this compelling.
Most (all?) LAIs on the market right now take some time to get up to therapeutic plasma levels with only a single injection. You can solve this in two ways:
Give the LAI plus keep the patient on PO medication for some period of time. This is what is typically done with haloperidol (Haldol) and certain forms of risperidone (Consta and Rykindo). For some, the duration of supplementation is very clear - Risperidal Consta requires 3 weeks of supplementation - but others it’s very much not. I’ve seen at least 3 different suggestions for PO haloperidol supplementation and nobody seems to agree on what is the best.
Add a loading dose injectable to rapidly increase levels. This is what paliperidone (Invega) and aripiprazole (Aristada) do, though each does it with slightly different mechanisms. Invega just uses two doses spaced close together (one fixed dose + one variable dose depending on PO equivalent). Aristada uses a special loading formulation called Aristada Initio that you give along with a single PO dose + your maintenance dose.
It’s nice that Uzedy is a one-and-done sort of thing.
To help me not feel like a slimy drug rep, I should point out a few things that I have gripes with (I plan to spend some more time on their primary study in a longer article.)
First, dosing only goes up to an oral dose equivalent of 5mg of risperidone, though most patients don’t actually need more than 6mg. It seems like you could just mix-and-match the smaller doses to make a higher dosage if you need it (if insurance will pay for it is another question).

It looks like 1mg of oral risperidone is the same as 25mg of Uzedy - it scales exactly how you would expect it to within the 1 month and 2 month dosing periods - so I don’t see why not, but this is purely speculative on my part.
The second thing is that it looks to me like they’ve set their therapeutic threshold a bit low. I reviewed a lecture on antipsychotic plasma levels that I put together and it seemed like the consensus was that 15ng/mL was therapeutic threshold - but Teva is saying that it’s 10ng/mL. I think this is probably just academic if the outcomes are comparable, but it warrants a closer look at the efficacy data.
These new features are due to what Teva is calling SteadyTeq. This article describes it as:
MedinCell’s BEPO technology—also called SteadyTeq—is based on copolymers and a biocompatible solvent that are formulated along with the active ingredient. After dosing, the ingredient is trapped in a depot that gradually degrades, allowing the drug’s slow release.
Copolymers! Biocompatible solvents! I don’t really know what that actually means, but it’s cool and I’m gonna use it. Also it’s already covered by MassHealth and NYS Medicaid which is actually pretty surprising. It must be enough of a cost-savings for them relative to the other LAIs for it to get onto their formularies so fast.
There were a few other novel therapeutics that some companies mentioned were in development that maybe I’ll write about soon. There was also an industry sponsored talk about the muscarinic agonists which makes wonder if they’re going to be hitting the market soon. Gotta warm the psychiatrists up for the first new therapeutic class for psychosis that might actually be effective since, uh, 1952.
Presentations:
Sorry, didn’t go to any so not much to say. Not that there weren’t some interesting looking talks! It’s just that, look, I’m not the sort of person who can sit still and listen while somebody talks at me for 90 minutes straight unless I’ve taken my Vyvanse. If Penn State didn’t record all of their medical school lectures and make in-person attendance optional, I probably wouldn’t have my MD.
I did try to go to one talk.
It was titled “Does Psychiatry Need a New Epistemology?” I was surprised to hear that someone thought psychiatry had an epistemology, let alone one that was old enough to need replacing (must be a very recent development, I thought) so I figured I’d see what they were on about. I noticed it was suspiciously marked as a DEI talk in the program and nothing else, but I assumed that they just needed to mark it as something so I went anyway. Then I walked into the event room, saw that it was all about the Maori conception of mental illness, realized that the talk should’ve been titled “Psychiatry Needs Another New Epistemology: It Just So Happens We Have One Right Here!”, and decided I should leave before I heard anyone unironically use the phrase “alternative ways of knowing.”
It was around this point that I remembered that I was in NYC - not in the eternal disappointment that is the Boston metro food scene - and proceeded to gorge myself:
Shanghai 21 in Chinatown for some great soup dumplings and a dish of stir-fried snap-pea greens that were incredible.
Zutto Ramen in Nolita - Good ramen, but mediocre chashu
Serafina’s - I did not realize there are 10 of these, but it was pretty good pasta. The burrata and fried artichokes were excellent
Frenchy’s Food Truck - Authentic French pastries out of a food truck in Brooklyn - I’ve been to Paris a handful of times, I’m very nitpicky about pastries, and I basically can’t tell the difference. I used to get a pain au chocolate every morning on my way to work when I lived in Brooklyn. David - a Frenchman - is one of the nicest people you will ever meet.
I continue to find NYC enchanting and I continue to forgive it for a level of dirtiness and general unruly behavior that I would never let another city off the hook for. I was a bit surprised to see just how open marijuana dealing has become. In Boston there are dispensaries everywhere, and it’s not unusual to see someone smoking a joint or a vape, but I generally don’t see people selling or rolling up on the street. In NYC I saw a dude rolling a joint on the subway, a group of people laying out what looked to be a full ounce of weed on a bollard, and then a group of Senegalese ?refugees who had two large kitchen storage containers filled to the brim with flower, and another with pre-rolled joints. Wild!
Oh yeah, I discovered the Silk Sonic album (a collab between Bruno Mars and Anderson .Paak). I realize I am 3 years late to this particular party, but I’m glad I got there.
Thanks for reading my diary/food blog/music review article - I’ll have actual technical stuff for y’all soon.
I’m sure that I have gotten some details wrong here. I don’t care.
I can’t figure out if this is somehow clever like AMbien or just supposed to sound like “u ready?” I give it a 5/10.
The Invega reps won’t tell you this, but RISPERIDONE MOLECULE can also transform into PALIPERIDONE MOLECULE. Truly there is nothing that Uzedy cannot do.
I was going to make a derogatory comment about NYC but after 22 months in Boston im just jealous that you had a weekend of good food.
Wish I read this before, I would have actually talked to the Uzedy people