


On Being a 3rd Year Psychiatry Resident

Since I’m about halfway through my 3rd year of residency (aka PGY-3) I thought it would be interesting to reflect on my thoughts about what my experience has been so far. Unlike my previous posts, this is not going to be a technical piece of writing.
None of these thoughts are in any particular order of importance, I just wrote them down as they came to me, and expanded on them to the point where it no longer felt particularly interesting. Might turn some of them into full essays, who knows?
Also, sorry, no internecine drama here - my department chair is a subscriber1.
Let me give my non-physician readers a little info about residency to put this into context:
Residency is best thought of as a medical apprenticeship. Everyone spends ~4 years getting through medical school, and then you “match” into a residency program which teach you the specifics of a particular specialty (e.g. psychiatry, surgery, OBGYN, etc.). During residency you are a doctor (i.e. you have a medical diploma and the letters MD or DO after your name), but cannot practice independently in most states2.
If you want even more specialized training within a field, you can do a “fellowship” which is essentially just another residency except for a particular sub-specialty. For some sub-specialties, this is really the only path into them - for example, if you want to become a rheumatologist, you first go through an internal medicine residency3 and then do a rheumatology fellowship. In other specialties, like psychiatry, fellowships are not really necessary.
Psychiatry residency is 4 years long, and though there are differences by program, seem to follow the same general structure. Again, there will be variations program-to-program:
PGY-1: You fulfill your 6 months of “off-service” rotations4 and do 6 months of hospital-based psychiatry (e.g. addiction, consult/liaison, inpatient psychiatry)
PGY-2: No more “off-service,” just psychiatry. Some programs (like mine) have you start seeing a small panel of outpatients in this year
PGY-3 (I am here): Primarily outpatient based. At my institution we essentially run our own private practice. We also rotate through different outpatient clinics5 and community-based programs.
PGY-4: More outpatient, but also you may step into a “chief” role where you learn the administrative side of running various services. This is also where residencies tend to stick elective experiences (e.g. neuromodulation, forensics, etc.) for residents who want additional exposure to particular parts of psychiatry.
After you finish PGY-4 year you are deemed “board eligible,” which means you can start practicing independently and obtain your final (required) certification by taking and passing “the boards.” You don’t actually have to do this right away - depending on your specialty you have between 3-5 years to take and pass your board exam.
General
First, I want to say that I am very happy that I went into medicine, and that I am particularly happy in psychiatry. There is a lot of doom-and-gloom about our profession generally, so as someone who is actually quite pleased with my career choice, I feel like I should say that.
PGY-3, at least at my program, feels like the loneliest year. I feel the most disconnected from the residency by far, I think because of how stark the contrast is between the required amount of interactions between yourself and your co-residents.
In first year you know just enough to be dangerous, so you’re always paired up with a PGY-2 and people are checking in on you constantly. You’re also bonding with your co-residents about how miserable your medicine months are, and how relieved everyone is that they didn’t decide to inflict that particular mistake on themselves.
As a PGY-2, you’re now responsible for your very own intern! I really enjoyed this role and find myself missing it a lot - this is part of what signaled to me how much I love teaching. You’re also exclusively working in psychiatry as a PGY-2, so except for the 2-3 months where we rotated outside of the hospital, you’re seeing your co-residents constantly.
In PGY-3 year, I suddenly find myself in the outpatient world, and I realize how lonely it is relative to the rest of residency. Most of my time is spent in my office seeing patients, writing notes, and dealing with administrative stuff. My co-resident’s offices are just a few doors down, but it’s surprisingly difficult to find time during the day when people are free to chat. Similarly, a bunch of the PGY-1 and PGY-2s are either just down the hall or a floor below me, but I worry about distracting them too much.
This year has given me perspective on what it would be like to have a private practice, and I don’t think I’d like it very much, at least not if it was all I did. For better or worse, I make a lot of my friends through wherever I work.
Outpatient Thoughts
Isolating or not, outpatient has been an immensely challenging, frustrating, and rewarding experience. I really do enjoy it!
Clinic Rules
It turns out that setting up rules for your clinic is hard. How many times should you allow a patient to not show up before you terminate with them? What’s an acceptable amount of notice that people need to give you in advance for cancellations? What are reasonable excuses? Not being a pushover with the patients you like is difficult. Not trying to get rid of people you don’t like is difficult. It’s hard when the only way to penalize patients who continually break the rules is to terminate with them. I can’t charge no-show fees.
Making sure you don’t overextend yourself is difficult too. Everyone wants appointments after 5pm, and some patients don’t work the sort of jobs that allow them to do anything other than after 5pm. We’re warned not to think of situations as “if I won’t, nobody will” - but in some cases it’s true! There just aren’t enough psychiatrists.
Some takeaways:
When you’re creating your clinic rules, be honest with yourself about how much of a squish you are. It’s true that it is easier to start strict and then loosen your rules with time, but this approach can also lead you to feel guilty about having applied strict rules to earlier patients and make it harder to be appropriately strict under whatever rules you currently use now.
Clinic rules are therapeutic when applied consistently. It’s easy to come up with reasons why you don’t want to have to enforce them, but I think you are doing yourself and your patients a disservice if you refuse to.
Doing Therapy
Learning to do therapy has been a very interesting experience. My first few months of outpatient felt very demoralizing. I was realizing all of the ways in which I was not terribly good at what I was doing (e.g. intellectualization is a hard habit to kick for me), and I didn’t feel like I was going anywhere with my patients. This resulted in me trying very hard to get better by reading/thinking a lot more about my methods. At some point in the past 2 months, though, I’ve started to notice small pieces of progress and it’s a wonderful feeling. Even for really small things! I have literally done little celebration dances after appointments in my office. Unfortunately, I got lax with my improvement work and am just now realizing it.
Supervision
Supervision6 is also a mixed experience. I have three different supervisors with three different therapeutic backgrounds (generally psychodynamic, ISTDP, and behavioral w/ a focus on ACT), who are all very smart, lovely people. I enjoy meeting with them to talk about my patients every week, deeply appreciate their perspective and advice about my psychotherapy patients, and then I proceed to forget 99% of what we talked about and do my own thing.
Part of me feels very guilty about this! My supervisors all have way more experience than me and probably know what they’re doing, so I feel like I should be trying much harder to take what they say and integrate it into what I do.
The other part is the one that has read Better Results: Using Deliberate Practice To Improve Therapeutic Effectiveness7, which makes the point that most psychotherapists actually become less effective over time (though more confident!). They also point out that things like therapeutic modality and quality of supervision actually contribute very little to how effective someone is as a psychotherapist. This makes me feel a little less guilty.
Billing/Coding
Learning how to bill for visits (aka “coding,” referencing the various CPT8codes), has made me feel like I am constantly committing fraud even though I know I am not. It’s just that billing codes feel very weird. There are two ways to bill for the E/M (evaluation and management) codes that are our bread-and-butter billing. Time and complexity. Time based is exactly what it sounds like, and there are billing tiers in 10 minute increments (10-19, 20-29, etc.). Complexity based billing is based on a number of things like “how many chronic illnesses did you address?” and “did you manage their prescription medications at the visit?” There are 4 levels of complexity9, and the codes for those levels are identical for certain time-based codes. For example, a level 4 encounter is also “moderate complexity” and is reimbursed the same as a 30-39 minute visit no matter how much time you spend.
The problem is that nobody gives clear answers about what the words ‘address’ and ‘manage’ in those sentences actually mean, so everyone just assumes a maximalist definition of those terms. There is also a very high rate of psychiatric comorbidity in psychiatry (e.g. people with generalized anxiety disorder are very likely to have other psychiatric illnesses), and so almost every patient we see has at least two “stable chronic illnesses,” both of which are easily ‘addressed’ (i.e. talked about) at the same time. If you happen to also discuss the patient’s medications in that visit, viola that’s now a “moderate complexity” encounter, even though it probably only takes a good clinician 10 minutes to do those two things. I feel like I am doing something vaguely criminal when I bill most of these patients as moderate complexity, because it feels like low complexity even though I can honestly say they meet criteria for moderate.
Clinical Scales
There seems to be no middle ground about whether or not people like clinical rating scales in psychiatry. People seem to think they’re either very necessary or are very stupid.
I feel like I’m the only person in the middle.
I really dislike the blanket use of clinical scales. Our hospital has mandated PHQ-9s for all patients with a diagnosis of depression, and I continue to be annoyed every time I am reminded about this despite the fact that I’ve chosen to use the Beck Depression Inventory (BDI) instead. ADHD scales I also think are generally useless unless I think the person filling it out really has no desire to be diagnosed with ADHD and I can trust them to not just rank everything as high as possible.
However, I’ve found that they are very useful if you treat them as the flawed tools that they are. Here are some reasons I like them:
Nobody has time to do a good interview at every appointment, and something like the BDI or PCL-5 is very time-efficient.
Scales often cover some nuance in symptoms that I would’ve definitely missed, and can help me notice symptoms that I otherwise wouldn’t have asked about if my impression during the interview had been trending away from a particular diagnosis.
Discovering discrepancies between how the patient appears and how they self-report can be very illuminating10.
Scales can help patients to better understand and verbalize their symptoms. It’s really nice when a patient can tell you more about what’s going on other than “I’m depressed.”
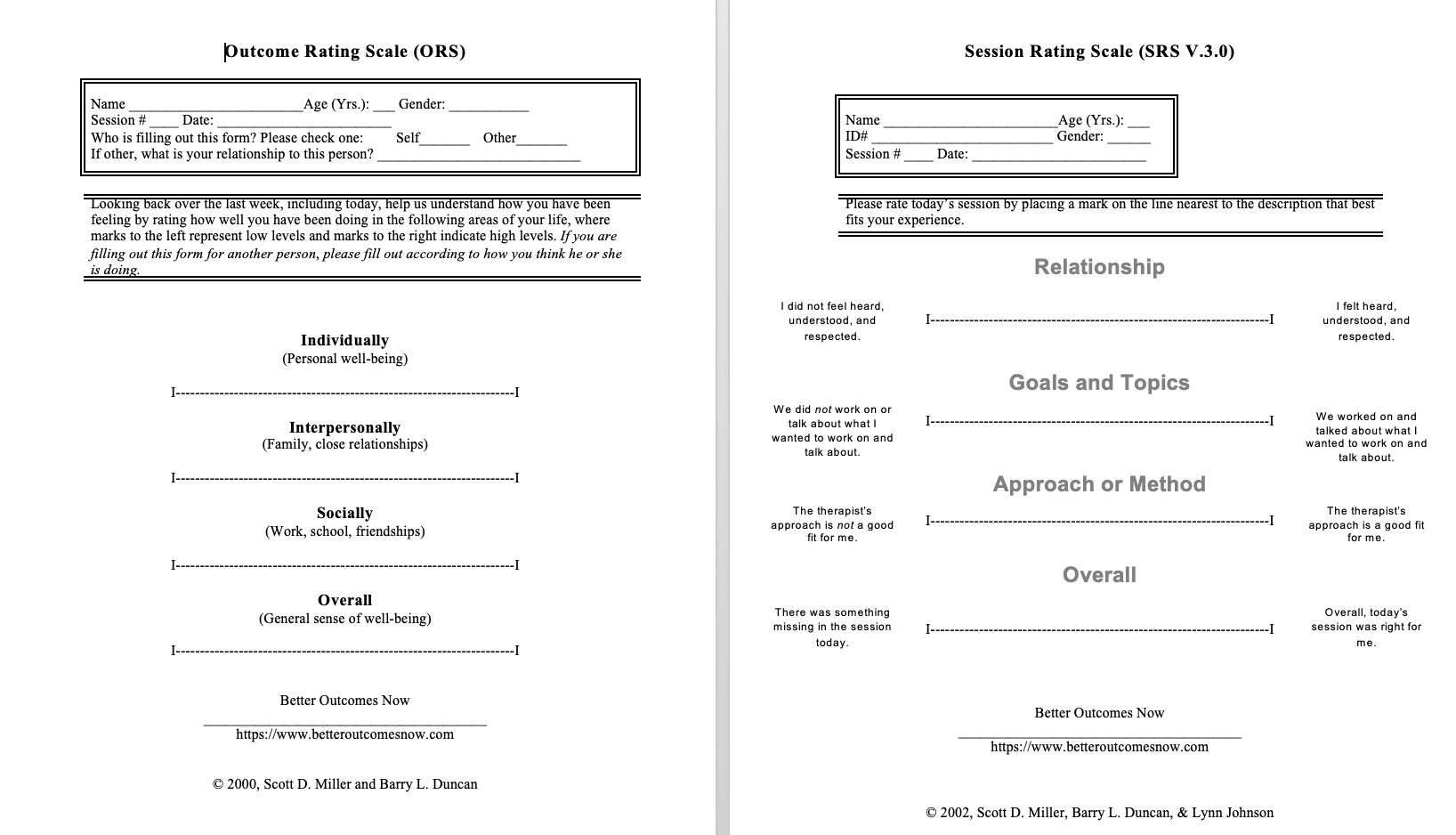
I also wanted to note that I’ve been using the Outcome Rating Scale/Session Rating Scale (ORS/SRS) from the Better Results book I mentioned above to help track progress with my therapy patients - check out the link to see what they look like. I’ve gotten good at consistently collecting it in-person, but not so good for virtual appointments. It’s helped me to have some good conversations with patients about what they think of as “getting better.” Still feels pretty difficult to have patients be honest about how well the different aspects of our therapeutic relationship are going - I consistently get very good scores on this count, but I am suspicious of them. It’s hard to criticize your doctor to their face, even when they are literally pleading with you to do so!
{kind=link}
Moonlighting11
Moonlighting has made me better understand why non-resident physicians come off to me as so absurdly risk averse sometimes. It’s difficult to accept the risk! You can tell yourself all you want that, once you’re an attending, you will make only the best, most rational, and risk-appropriate decisions and never once shall you waiver from this path.
Haha, no, you will absolutely do that.
There really is no substitute for knowing that, this time, the buck really and truly stops with you. There is no attending who you can trust to know better, no more excuse that “I’m still in training.”
I had this experience just recently when I was called to examine a patient with a history of heart attacks who was complaining of chest pain. Her symptoms were totally consistent with getting roughed up by police a few days ago, not at all with a heart attack, but there was still a small piece of my brain screaming JUST SEND HER TO THE ED, TO HELL WITH YOUR IDEAS OF RESPONSIBLE RESOURCE UTILIZATION. TALK TO ME ABOUT UTILIZATION WHEN THE PATIENT DIES AND YOU CAN’T UTILIZE YOUR MEDICAL LICENCE ANYMORE, IDIOT. AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAA.
I am proud to say that after careful consideration of that point of view (and some extensive risk/benefit conversations with the patient) I was able to politely, but firmly, tell that voice that while I appreciated its thoughtful commentary on the situation, the prefrontal cortex has decided to go in a different direction at this time.
I don’t want to be too self-congratulatory here, because my real takeaway was not so positive. It’s clear to me now that, at some point, that scream coming from somewhere in the Risk Avoidance Department of my amygdala is going to win; even when it shouldn’t. I’m going to be too overburdened, or too tired, or too uncertain or whatever, and some EM doc in some ED is going to go “these goddamn psychiatrists can’t even read a goddamn ECG,” though at least on that count they will be pretty correct.
My point here is twofold. First, don’t underestimate the Risk Avoidance Department. Second, just because the Department might win sometimes doesn’t mean that we shouldn’t try and adjust and continue doing what is right instead of being afraid.
Whether or not he reads this is another question
The caveats to this get complicated and are state dependent! In MA, for example, you can get your full license to practice after 2 years of residency training, but most places will not hire you unless you’re on the path to becoming “board certified,” meaning you are/will be accredited by the national board for your specialty.
You can think of this as a general medicine residency, though usually more focused on hospital medicine than something like a family medicine residency.
For us this was 2 months of neurology, 3 months of medicine wards, and 1 month of emergency medicine
Geriatrics, pediatric consult clinics, forensic clinics, a primary-care consult clinic, etc.
i.e. Outpatient and therapy supervision, where MD’s and PsyD’s oversee your outpatient and therapy work.
Probably worth a book review.
Current Procedural Terminology
Level 1 doesn’t exist. Level 2 is the lowest, level 5 is the highest
e.g. I had a patient self-report extreme edginess and high startle response on the PCL-5. A few minutes later, a door outside creaked and she gasped and turned around to look behind her. After seeing that my office door was closed, she turned around with a sheepish grin on her face and said “Sorry! I thought that there were kittens!”
Working at other hospitals outside of my residency as an independent physician for experience and extra pay.