
Wot's... Uh The Deal with Trazodone?

At the beginning of my psychiatry residency, I was wonderfully ignorant about sleep aids (as well as other things, but those are for other essays). My knowledge of treating insomnia (Onset? Maintenance? Same thing, right?) consisted of my personal experience being prescribed amitriptyline and trazodone, trying OTC melatonin but being disturbed by the weird dreams, and then giving up before asking my doctor to prescribe me one of the “z-drugs” (the ‘z’ usually goes at the beginning, like in zolpidem and zaleplon, but as long as its near the front that’s ok too like with eszopiclone). I gave up because: I knew that I hadn’t actually worked on my sleep hygiene and felt vaguely bad asking for a pill to fix it. Anything that acts on GABA receptors is fretted over by physicians as a possible drug of abuse and I didn’t want my doctor to think I was drug seeking. Most importantly, I felt unprepared to meet the Ambien Walrus.
A few months into my first year of training, I realized that I should probably start learning about how to properly address insomnia considering something like 100% of my inpatients requested a sleep aid at some point during their admission. Up until that point, I had just been using trazodone because it was the only non-benzodiazepine, non-z-drug in our admission order set. Unfortunately, for my free time - and yours, if you’re reading this - I have a very healthy distrust of default options in medicine after finding out that the laxative docusate has been studied in multiple RCTs that fail to differentiate from placebo and yet the WHO continues to list it as an “essential medicine.”
The place I started was with the American Academy of Sleep Medicine’s (AASM) clinical guidelines for treating chronic insomnia1 in adults, since they seemed like the sort of people who would know about this sort of thing. In their abstract I was graced by this very straight-forward set of recommendations:


Trazodone is/was the most commonly prescribed sleep aid I see, and it’s not even close. I just spent a few minutes trying to remember the last time I saw a patient complaining of insomnia that wasn’t already on trazodone and I literally cannot think of one. Before you ask, yes, I did notice the word “WEAK” over and over again at the end of all of these suggestions, but I figured that if everything else is also WEAK, it was better to follow a WEAK positive recommendation from the AASM than a WEAK negative recommendation so I started using doxepin instead.
I thus attempted to evangelize the Good Word of the AASM to my attendings and co-residents, but then they would say very reasonable things like, “I’ve been using trazodone for decades, nothing bad has happened, and patients seem to think it works,” and, “nobody sleeps well in the hospital, it probably doesn’t matter what you give them anyway,” and “hey aren’t there some studies that show it preserves sleep architecture?” My responses to these questions felt WEAK because of my WEAK understanding of the literature, and so I decided to wade into the depths of the psychopharmacology literature to fulfill my Jungian Hero’s Journey and become the sort of man who can make STRONG recommendations instead.

Trazodone and the Mental Pain Model Of Depression
Trazodone was first synthesized in 1966 by Bruno Silvestrini2 and another Italian by the last name of Palazzo whose first name I can’t be bothered to find. Silvestrini wrote extensively about the “mental pain” model of depression, in which he argued that the mechanisms responsible for psychic pain are the same as the ones responsible for somatic pain. He hypothesized that patients with depression had a lower pain tolerance than the rest of the population, and that medications that could modify that might work as antidepressants. So, Silvestrini and co. decided to try and find a drug that would antagonize the α1-receptors, which were known to be involved in the pain circuitry of the CNS.
Thus, trazodone, a strong α1 antagonist was born and, hey, it worked as an antidepressant. The FDA approved it for the treatment of depression in 1981, its unique mechanism of action cured millions of patients with MDD, Silvestrini’s Mental Pain Model was vindicated, and psychiatric trainees are required by the APA to hang a picture of him above their call room beds to this day.
Just kidding, mostly.
The FDA did approve trazodone for depression in 1981, but trazodone is almost never prescribed for anything other than insomnia, and Silvestrini’s Mental Pain Model is nowhere to be seen in modern psychiatry3.
It turns out that while trazodone has high affinity for alpha-1 as an antagonist4, it also has high affinity for a bunch of other receptors and monoamine5 transporters. Alpha receptors are really important in allowing your blood vessels to constrict in response to changes in position to ensure that your brain continues getting enough blood. When we sit or stand up, our sympathetic nervous system recognizes the change quickly6 and squirts out a little extra norepinephrine, which binds to alpha receptors causing the smooth muscle in your blood vessels to contract and shunt more blood to the brain. Without this compensatory response, we’d constantly have the experience of standing up, feeling light-headed, having our vision get a bit fuzzy, and maybe even passing out.
Ok, that’s as close as I want to get to cardiology for the next 6 months. Let’s get back to the psychopharm.
This paper7 simulated the predicted receptor/transporter occupancy for various doses (50mg, 100mg, 150mg) of trazodone. The 150mg dose, which is the lower bound of trazodone’s antidepressant dosing range is right around the point where it starts to block serotonin reuptake to the same degree that the SSRIs do, and at progressively higher doses it (presumably) begins to significantly block norepinephrine reuptake. This suggests to me that it’s probably just doing what the SSRI/SNRIs do for depression and there isn’t anything unique about it.
Looking at the rest of the occupancy data, we see from a theoretical point of view why trazodone might be effective for sleep. Straightforwardly, it’s a potent antagonist at H1, with ~84% of receptors occupied at just 50mg. This lines up with H1 receptor occupancy for other medications with H1 antagonism at doses that we use for sleep. For example, an in vivo study found that 2.5mg of olanzapine blocked between 61-80% of H1 receptors, and 25mg of quetiapine blocked 56-81%. Alpha receptors and 5HT2 receptors also seem to promote wakefulness, so their blockade likely contributes as well.
The AASM Guidelines Revisited
I decided to go back to the AASM paper and look more closely at their WEAK recommendations.
Before I get into it though, I want to point out something that they did which I thought was a good idea, which was to set clinical significance thresholds.
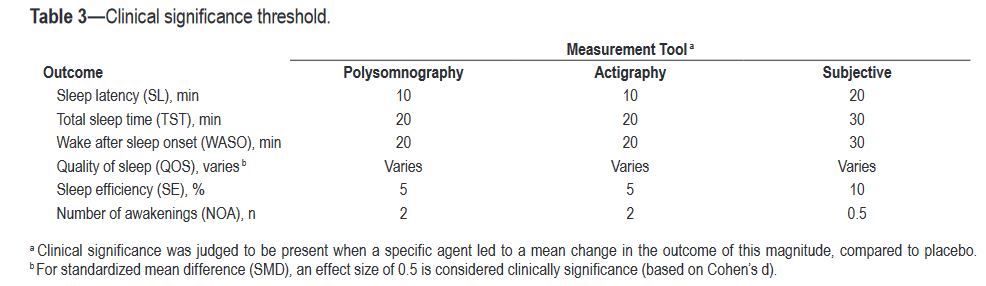
I think we get a little too excited about small p-values when the real-world difference is so small that neither you nor the patient will notice anything other than the monthly copay.
I am unsure about how the AASM arrived at the numeric thresholds that they selected - my hope is that they correlate with positive outcomes. They do seem to be in line with the size of the changes seen in the studies I’ve reviewed, but I’m a little skeptical that an additional 20 minutes of sleep is clinically significant. This is probably because I don’t have a great sense of how much these numbers tend to translate into objective improvements elsewhere in life, but as a life-long sleeper I think I am able to argue this point at least a little bit. The one exception is their cutoff for number of awakenings, which is actually pretty aggressive - no drug they report even gets close to two8!
I am less thrilled about this weird “Patients’ Values and Preferences Assessment” that seems like it’s just the authors guessing about whether or not a majority of patients would use a medication over no treatment. It results in odd things like them saying that doxepin’s benefits outweigh the harms, and trazodone’s harms outweigh the benefits, but then saying about both that “The majority of patients would use this treatment (over no treatment), but many would not,” and then recommend using one but not the other.

I went back to the AASM paper and looked at the section in which they discuss how they came to their conclusion for trazodone, and… oh huh there’s just one study they cite which is Walsh et al, 1998. I knew that couldn’t be correct, I had seen at least a couple more at that point, so I went to every paper’s most important and yet most studiously ignored section - The Methods - to see their exclusion criteria.

These criteria might seem excessively narrow, but if you’re the AASM, writing primarily for sleep specialists, they make a lot of sense. Insomnia is a super common symptom seen in many other conditions (e.g. depression, stroke, terrible pain all the time), and so you can see why they would want to focus on primary insomnia because things like depression and terrible pain all the time are not the sort of thing that sleep doctors are supposed to be responsible for solving.
If you’re a psychiatrist like me, though, clinically significant insomnia tends to be part-and-parcel with our most common psychiatric illnesses so I don’t particularly mind if a study examines patients with comorbid major depressive disorder. Unfortunately, this means that the AASM criteria are much too narrow, which is why the rest of this essay exists.
What is “Insomnia”?
Insomnia is both the domain of psychiatrists and sleep medicine docs, so there are two slightly different definitions depending on which diagnostic manual you use. For our purposes they’re basically the same definition, so I’ll just outline the criteria:
Difficulty initiating or maintaining sleep
That results in significant daytime consequences
Lasting least 3 days a week for at least 3 months in duration
Not better explained by environmental circumstances (e.g. using a lot of cocaine), or another condition (e.g. major depressive disorder)
The AASM paper above estimates the prevalence of chronic insomnia between 5-10% in the general population, though 30-50% of the population will meet these criteria for periods of time less than 3 months intermittently throughout their lives.
How We Measure Sleep
At this point we have to talk about how we measure sleep and what the terms I’ll be throwing around mean. Sleep medicine gets a Gold (has been downgraded to) a Silver Star for (mostly) avoiding inscrutable technical language.
Objective Measures
Total Sleep Time (TST) - Is exactly what you think it is. It starts when you are no longer conscious9, and ends when you wake up without trying to go back to sleep.
Sleep Latency (SL) or Latency to Persistent Sleep (LPS) - The time it takes you to enter sleep after you start trying to fall asleep. A normal SL is 10-30 minutes.
Wake After Sleep Onset (WASO) - The amount of time you spend awake after initially falling asleep (e.g. if you fall asleep, wake up, and spend 30 minutes tossing and turning before you eventually get back to sleep, then sleep through the rest of the night, your WASO is 30 minutes). A normal WASO is <30 minutes.
Number of Awakenings (NAs) - Also exactly what it sounds like. Just kidding, this is actually confusing because the sleep literature seems to make a distinction between awakenings and arousals and then authors use whatever terms they feel like depending on the paper.
Best I can tell, awakenings refer to events in which the person is subjectively aware of the fact that they are awake. A few10 of these a night are normal in healthy individuals
Number of Arousals/Arousal Index (Also NAs/ArI) - Arousals are defined11 as:
An abrupt shift in EEG frequency, which may include theta, alpha and/or frequencies greater than 16 Hz but not spindles, subject to the following rules and conditions: [click the link for the following rules and conditions]
These are significantly more frequent than awakenings, and are measured by the Arousal Index, which is the number of arousals per hour. This paper looked at ArI’s in normal individuals and found that a normal ArI increases with an individual’s age, with a mean of 10 in the 18-20 age group, up to 21.9 in the 61-70 age group.
Sleep Efficiency (SE)- Percentage of time spent asleep while in bed (e.g. if you fell asleep as soon as your head hit the pillow, and then get out of bed as soon as you’re done sleeping, that’s 100% sleep efficiency). A normal SE is ≥85%.
All of the above parameters can be measured objectively. The gold standard is the polysomnogram (PSG) - in which your heart rate, blood oxygen, EEG activity, and other things12 are monitored. Another method is called actigraphy, which is basically just a very sensitive accelerometer that you wear on your wrist13. One of these things does not sound like the other, but it turns out that actigraphy is actually pretty good at measuring TST, WASO, and NAs relative to PSGs.
Subjective Measures and their Problems
You can also have patients self report things like TST, NAs, etc. Unfortunately, and unsurprisingly, people are not very good at doing this. The CARDIA Study asked 647 people to estimate their sleep, while using concurrent wrist actigraphy to determine their accuracy. Young, old, male, female - doesn’t matter who they were, people were pretty uniformly bad at estimating their actual sleep time. I’ll just quote the study:
Average measured sleep was 6 hours, and subjective reports averaged [48 minutes] longer than measured sleep. Subjective reports were not well calibrated, increasing on average by 31 minutes for each additional hour of measured sleep14. Our model suggests that persons sleeping 5 and 7 hours over-reported, on average, by 1.3 and 0.3 hours respectively. Overall, there was a correlation of 0.45 between reported and measured sleep duration.
Note that the average discrepancy here is longer than the AASM’s clinical significance threshold for TST of 30 minutes for self-reported measures! In my mind, this totally disqualifies any study that attempts to rely exclusively on patient self-reports of objective sleep data like TST, WASO, etc.
Sleep Quality (SQ) - Is an inherently subjective assessment and uses questionnaires, the most popular of which is the Pittsburgh Sleep Quality Index (PSQI). It asks ‘objective’ questions like “during the last month… how many hours of actual sleep did you get at night?” but also asks subjective questions like “How would you rate the quality of your sleep over the last month?” and “how often have you had trouble staying awake while driving, eating meals, or engaging in social activity?”
Others include the Leeds Sleep Evaluation Questionnaire (LSEQ) and the Epworth Sleepiness Scale (ESS).
Unfortunately, the PSQI and the LSEQ rely heavily on self-reported sleep measures. Nine of the PSQI’s 21 points are entirely based on self-reported sleep data!
On some level, we shouldn’t care about a patients’ subjective experience regarding the quality of their sleep. There is plenty of evidence out there about how insufficient or poor quality sleep effects cognition, reaction time, etc. and how there seem to be poorer long-term consequences for people who don’t get enough sleep.
The pragmatic part of me knows that these things obviously do matter, because typically patients with insomnia are coming in because of subjective issues they are having during the day or because of the distress they experience when they wake up at night.
I was curious to know if changes in PSG/actigraphy data matches up with subjective improvements in functioning and it mostly seems like this is not the case? I couldn’t find any meta-analyses on this specific question, though I’m sure they exist. As we’ll see, though, almost every individual study for trazodone that shows statistically significant improvements in SQ does not find the same for objective measures of sleep.
Walsh et al.
This is a good study to walk through before I talk about some of the meta-analyses and literature reviews because I think it reflects how low-dose trazodone probably “works.”
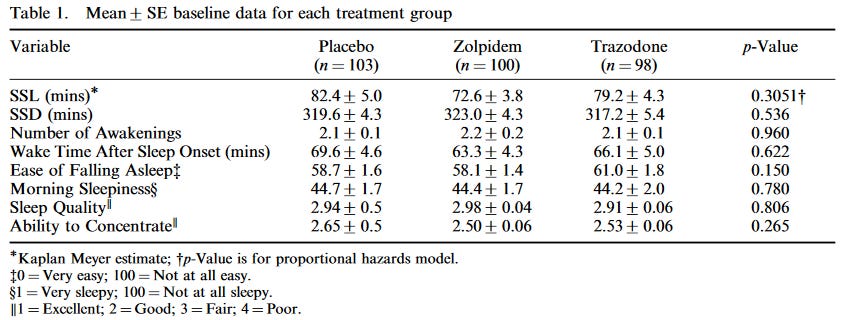
Walsh is a randomized, double-blind trial in individuals with a diagnosis of primary insomnia. Patients were randomized to placebo (n = 103), trazodone 50mg (n = 98), or zolpidem (aka Ambien) 10mg (n = 100) for 14 days. They were asked to self-report SL, TST, WASO, and NAs. They were also asked to report the degree to which their sleep problems was causing problems in their life, SQ, ease of falling sleep, morning sleepiness, and ability to concentrate.
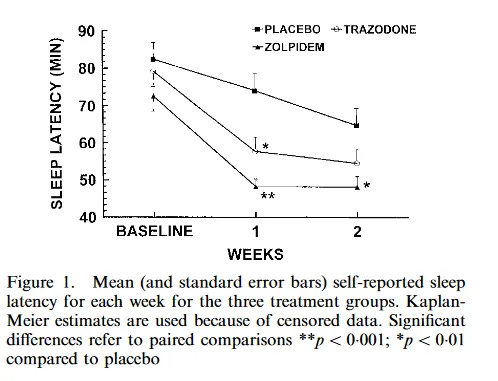
The primary outcomes were self-reported TST and SL, both of which showed separation from placebo at week 1, but not week 2

Some secondary outcomes similarly showed effectiveness at week 1, but not at week 215

But when patients were asked about their overall impression of the effect of the treatment, there was sustained separation at both week 1 and 2 for certain categories.

The biggest gripe I have here is that there is no data included for patient evaluation of “the disruption caused by the sleep problem on their work, social life, and family life” via the Sheehan Disability Scale. The authors simply say:
No significant differences were observed among the groups with respect to the patient distribution in these categories at baseline or at any time of treatment. This was expected as the study was not powered for this outcome measure. At baseline, approximately 88 per cent of the patients felt that their sleep disturbances disrupted their work, social life, or family life to some extent. This percentage fell to between 70 and 75 at treatment week 2, regardless of group.
This is really frustrating, because it’s probably the most important outcome in the entire study! I also suspect that the authors wouldn’t have excluded the result if it came out that there was a significant difference here, otherwise why include it? I’m also kinda confused as to how this study wasn’t adequately powered to detect a difference here on a scale with a much higher resolution (1-10) than their SQ scale (1-4).
There was also no difference in morning sleepiness, and the “ability to concentrate” measure isn’t even mentioned in the results.
Anyway, how do we explain the study results here?
Basically, I think it comes down to the subjective effects of the medications and the effect on participant’s subjective experience around sleep. I can’t comment on zolpidem, but I have taken trazodone and it does a very good job at making you feel sleepy and even a little bit woozy the first few nights that you take it.
My best guess is that patients take these medications and notice that trazodone makes you feel sleepy, which causes them to overreport their improvements. In a week or so, when their bodies have adjusted to the effects of the medication and the subjective effects are less, it doesn’t bias the self-reports as much and so the statistical differences start to disappear.
Edit: Actually, I don’t think this quite works as an explanation, and needs a bit more nuance. The loss of significance in the TST and SL numbers are mainly due to improvements in the control group as opposed to as loss of effect in the treatment groups. This doesn’t mean that subjective effects can’t bias the reporting, but my hypothesis that the loss of significance is due to those effects wearing off should result in those groups moving back towards baseline which doesn’t happen here.
There are other results here that point out the oddities of how the authors decided to do self-reporting on sleep. For example, the difference in SL between trazodone and placebo at 2 weeks was just 10 minutes, but there continued to be a statistically significant difference between the groups in subjective responses to how quickly patients felt they fell asleep.
Overall, I think this is a bad result for both trazodone and zolpidem, and suggests that patients are probably responding to the subjective effects of the medications that they experience while awake, even without any measurable improvements in their actual function.
Let’s Get Meta
Let’s be fair though. Walsh is just one study, and we all know that meta-analyses are the gold standard for evaluating efficacy and there is absolutely nothing that should convince you otherwise.
Zheng et al. 2022
This paper is a meta-analysis of RCTs that looked specifically at PSG data. Its inclusion criteria allowed for studies of primary or secondary insomnia, that used trazodone alone or in combination with other therapies, for at least 1 week.
In general I think these criteria are fine for psychiatric purposes, since we’re mostly seeing secondary insomnia anyway and our patients are likely to be on other treatments that we know already modify sleep architecture like antidepressants.

It’s worth walking through some of these studies, because there are some oddities that pop up. Before I do, though, I should be transparent about the fact that I am generally extremely suspicious of any studies that are exclusively out of China because of the well known problem of “paper mills” and other fraudulent behavior in Chinese academia generally. To be clear, I am not suggesting papers from countries other than China are immune from fraud and other types of dishonesty - I have personally worked in a lab where one of my colleagues was discovered to have been falsifying data - but it is nowhere near the same magnitude as China16.
The Cao, Zhang, Wang, Chen, and Li papers are all studies conducted in China and account for 55% of their pooled subjects. I’m sure readers will be shocked to hear that this significantly lowers my confidence in this study’s results.
Cao et al., 2018 - Is mostly interesting to me because of this Flupentixol-Melitracen combination. Flupentixol is an old antidopaminergic that I’ve never actually seen used. Melitracen is apparently a tricyclic antidepressant (e.g. amitriptyline) that I have never heard of before, and appears to only ever have been sold in combination with flupentixol by Lundbeck starting in the 1970s under the brand-name Deanxit, but also under other more delightful names like Mocalm and Placida.
Haffmans and Vos, 1999 - I’m pretty sure that meta-analyses regularly exclude studies with very small sample sizes to avoid the problems that underpowered studies cause. However, this slide set that I came across suggests that this may not be a problem if you exclude small studies that are at high risk of bias - I don’t think they did that here, though.
Brofaromine is another drug I have never heard of because it never made it to market. It is a reversible MAO-A inhibitor, and according to this abstract had similar efficacy to the other MAOIs but without risk for tyramine-induced hypertension. I’m actually a little upset about learning about this, because having a MAOI that doesn’t come with dietary restrictions and is clearly as efficacious as the two currently on the market would actually be quite nice!
Chen et al., 2021 - This is the only one of these studies where the comorbidities feel like they should be exclusionary. Obstructive sleep apnea (OSA) is literally a problem where the fleshy bits in your mouth and throat block off your airway. I think that this is a problem that is different in-kind from the other comorbidities where the problem is probably happening in the brain itself.
Li17 - THIS IS A DISSERTATION! Even worse, there’s no link to the dissertation itself. I’m pretty shocked that this was allowed to be included in a peer-reviewed article, and it lowers my trust of the authors even further.
Let’s take a peek at the results in Table 2.

Before running through the significant results, I should just point out how crazy high the heterogeneity is here. Percentages in the 90s indicates that these studies are so different from one another, either in methodology or patient population, that <10% of the differences in the data are thought to come from random chance! The authors do try to explain this to varying degrees of success depending on the outcome, which I’ll touch on below.
TST - Very high heterogeneity, and the authors can’t find an explanation with sensitivity or subgroup analyses. Also, the Cochrane risk-of-bias tool for randomized trials that the authors used indicated a high risk of bias for the majority of the studies used in this outcome, and ultimately dubbed the certainty of the evidence “very low.” I would just call it WEAK, but I think we agree either way.
LPS (aka SL) - The heterogeneity here is crazy high, but the authors found that eliminating the Zhang et al. study reduced I^2 to 10%. New results were: MD = −9.85 min., 95% CI −15.34 to −4.37, P = 0.0004. Even if this is real, I don’t think that a 10 minute reduction is clinically relevant.
Interestingly a dose-based subgroup analysis found a much stronger effect for doses ≥100mg, and that the heterogeneity disappeared with this sort of stratification. The Zhang study is in that ≥100mg group, which makes me suspicious, but I’m not sure I have a good reason to be. Reducing time to fall asleep by ~40 minutes is actually quite good, though. I think this is their strongest result, though it’s rare that we get above 100mg for insomnia treatment with trazodone, and you have to wonder if the improvement is just because you’re at an antidepressant dose.

N1 Sleep - This is the lightest stage of non-REM sleep, and the stage from which you are most easily roused.
This is the first result reported as SMD. The authors did this because some studies reported change in some outcomes as a % change relative to baseline and others reported change in minutes. I looked at a few different sources and they indicate that N1 sleep accounts for 2-5% of total sleep time.
Heterogeneity was high here again, though a sensitivity analysis showed that this was driven almost entirely by the Stein et al. paper. When removed I^2 dropped to 2%, SMD = −0.86, 95% CI −1.25 to −0.46, P < 0.0001. This is also pretty decent, and the studies this result depends on are not Chinese except for one, so this also seems like one of their better supported results. However, given how small of an amount of time N1 sleep accounts for, 0.86 of a SD is probably going to be pretty small.
N3 Sleep - Highly significant, but with very big statistical problems. First, you’ll notice that this is the only result where the Egger’s Test - which looks for publication bias - is <0.05, indicating that the smaller studies have disproportionately large effect sizes. However, this statistic can be influenced by high heterogeneity which is certainly present here with an I^2 of 93%. Unlike LPS and N1, though, the authors couldn’t find a good explanation for the heterogeneity in this study and neither can I.
This is unfortunate because a SMD of 1.6 is probably a pretty significant change in overall sleep architecture if true. 10-15 percent of sleep is spent in N3.
I would also like to tentatively point out that in subgroup analysis, the effect only exists in studies that dosed trazodone above 100mg.
“NAs” - The most statistically significant result in the whole thing, finally without a ridiculously high I^2. Glancing through the studies though, there’s an issue with nomenclature. The authors of the meta-analysis use the term “number of awakenings,” but that’s not consistent with the studies themselves.
Take Kaynak which is included in the NAs analysis. Although Kaynak’s authors call this measure “# awakenings” the mean number of these range from 10-30 times a night, and they define them as <15 seconds of alpha-wave activity which seems like it is a measure of arousals. To contrast, Stein is also included, but explicitly uses an arousal index measure (which you can easily calculate number of arousals from), but in that study the mean ArI was ~10 which translates to ~50 arousals a night, way different from Kaynak.
This might just boil down to me quibbling about nomenclature (Nope it didn’t!) but I still think it indicates a sloppiness on the part of the authors that overall makes me pretty wary.
Anyway, assuming that the results are real, I’m not sure whether or not a SMD of -0.67 is clinically meaningful. It seems like it translates to somewhere around 6-7 fewer arousals a night.
WASO - No heterogeneity(!) but barely significant. Again hard to tell what this means clinically because it’s a SMD, but it seems to be roughly a 10 minute improvement which is unimpressive.
My takeaway on Zheng is mostly negative. From a big-picture perspective, the study has a lot of issues both in the studies it relies upon (again, there was a dissertation. I cannot get over this), and in its statistical results. I don’t think the results in TST and N3 sleep can be trusted.
The SL and N1 results suggest an effect at doses >100mg, which might predispose me to pushing the dose a little higher than I normally would in patients who appear to respond.
Yi et al., 2018
This is a meta-analysis of 7 RCTs in patients with primary or secondary insomnia, where trazodone was compared against placebo. Both objective and subjective data were permitted.

I think it’s pretty interesting that many of these studies were not included in the Zheng analysis above. It’s also quite interesting that these authors (who are almost all based in Chongqing, China) did not include many of the studies in the Zheng paper, and did not include any of the Chinese studies.
The whole “what is a NA really?” question is back again. I thought that maybe this time it seems that the ‘A’ means awakenings, because this paper only took SE, TST, and SQ results from the Stein paper even though you could easily compute the number of arousals if you wanted to. But then I noticed that they included the Kaynak 2004 paper which defines NAs as “alpha-activity < 15s” and the Roth 2012 paper which defines them as “one or more continuous, [30 second] epochs scored wake.”
Basically I think this means that these NA analyses are totally nonsensical and can’t be trusted until someone can explain to me how I have horribly misunderstood this concept.
In their conclusion, the authors say “trazodone was an effective and well-tolerated hypnotic for those patients with primary and secondary insomnia.”
‘Effective’ is not the word I would use here.
They showed - just barely - an increase in sleep quality (p = 0.05) per the PSQI self-report. Without a breakdown of what parts of the PSQI improved - remember, the PSQI has a lot of scoring questions that are dependent on self-report of things like SL, TST, etc. - I don’t think that a barely significant result means much.

Their other primary outcome of SE, as well as secondary outcomes of SL, TST, and WASO were not statistically significant.
The result for NAs was statically significant but I don’t think I need to copy-paste what I just wrote about how questionable this analysis is.
Everitt et al., 2018
This study is actually a Cochrane review of the effectiveness of antidepressants writ large for the treatment of insomnia, but they do have some data on trazodone. Interestingly they knew about they existence of the Le Bon paper used in Zheng but declined to include it in pooled analysis because “it did not provide sufficient data for it to be included in the pooled results.”
Their only significant results are subjective. The first is a barely significant improvement in SQ, basically the same as in Yi et al.

…though for some reason they felt Roth could be included, when the Yi authors felt otherwise.
The second is a reduction in the subjective number of awakenings, based on two studies, which showed MD -0.31, 95% CI -0.52 to -0.11
…is it always like this?
I started this journey by reading the AASM guidelines, thinking that trazodone had one study, poor evidence for its use, and deciding not to use it. Now I have discovered that there are plenty of studies, but the meta-analyses are garbage or show differences that I don’t think are clinically relevant.
For those wondering, the data doesn’t seem to be like this for other sleep-aids. For example, here is a study on low-dose doxepin that shows large PSG improvements in TST and WASO that are accompanied by significant and sustained improvements in subjective measures of daytime functioning all the way out to 12 weeks. Here’s a systematic review on the rest of the doxepin literature that features multiple, large studies. There’s also this very detailed network meta-analysis from the Lancet in 2022 that I have not read though entirely.
The big question I’m left with - which I didn’t think was wise to shove into this already long writeup - is to what extent changes in things like SL, TST, etc. translate into subjective wellbeing in the patients taking them.
I think it’s good to be specific about how I think this will/will not change my clinical practice:
I will continue to not prescribe trazodone for patients with insomnia unless they are already on it.
If patients are already on trazodone, and feel it is effective for their ability to get to sleep, I will be moderately more likely to increase the dose to see if they get more of an effect.
I do not feel that the negative evidence here is strong enough to de-prescribe trazodone in most patients who find it effective.
They don’t have an short-term insomnia guideline, I checked.
His last name would make a good name for a gin martini
At least, not explicitly so. There are some indications that Ketamine’s MoA is reliant on its opioid-receptor activity.
Incidentally, this makes me wonder if, like the SNRIs, trazodone could be useful for individuals with comorbid pain, but I’m not sure that it’s ever been tried.
dopamine, serotonin, epinephrine, and norepinephrine
Yes I know it is more complicated than this with baroreceptors and blah blah but I’m a psychiatrist, be glad I even remember what a baroreceptor is.
Another paper did a similar simulation, but showed very different receptor occupancy. Some of their data makes more sense - like significant SERT blockade not showing up till 300mg, but some make less sense, like how they have a higher Ki for H1 than the study I rely on in this article, but somehow find a much lower H1 receptor occupancy even at 300mg. Someone is wrong here, but I do not have a sophisticated enough understanding of these models to figure out who.
Zolpidem appears to get the closest, with a SMD of -0.95 awakenings.
There are fancy definitions that use brain waves but no need to get overly technical when it doesn’t matter.
The sources I’ve found are inconsistent on exactly how many are “normal.” Some say 2-3, others say every 90 minutes or so of sleep, which is about 4-5 for 7h of sleep.
Unfortunately, many papers seem to make up their own definitions of how this is scored - you’ll see.
Limb movements, facial muscle movements, eye movements, heart rhythm, a bunch of breathing parameters (I am sad I cannot do another footnote here as a joke) like airflow and respiratory effort. Hilariously, it was standard to monitor for “nocturnal penile tumescence” by placing “a band of paper tape with perforations (similar to coil postage stamps) that is fit snugly around the shaft of the penis and will break at the perforations during penile tumescence.”
This is how things like Fitbits track your sleep, though they also have O2 sensors and HR monitors.
I don’t think I understand what this phrasing means. Clearly it can’t be that people overestimated each hour by an additional 30 minutes, otherwise people who slept for 7h would be much worse estimators than people with 5h of sleep, but that's not the case.
As an aside I don’t understand how this “paired comparison” for a p-value works. Shouldn’t there be separate values for trazodone and zolpidem separately?
I really do not enjoy having to take this stance, but I don’t know how I solve this issue for myself other than to meticulously comb through every Chinese study for fraud. If anyone could provide me with some other way to do this in the comments, it’d be appreciated.
The table says et al. but the bibliography attributes to a single individual.
OH MY GOD. Are you ever hilarious. Wish you were my shrink. Love your cats.
I take An SNRI and if I don’t take 50 mg of trazodone at bedtime I can’t sleep. I am not an insomniac. My sleep is great. I’m on duloxetine and would love to discontinue however the symptoms are hard to bear so I keep taking it. Doing somatic stuff and meditating has pretty much handled the so-called depression
. AGH.
I really enjoyed this! As a patient, I was prescribed trazadone for insomnia but didn't take it much because i felt terrible the next day (worse then losing a couple hours trying to fall asleep). I also found the ACSM guidelines and showed them to my primary care, and he basically said "look, everyone's been prescribing trazadone for insomnia forever, why would I trust these guidelines that seem to push benzos and have nothing above low confidence in any recommendation".